From Coronary CT to functional maps and Ischaemic Burden* in minutes
fast, explainable AI, providing pragmatic analysis to clinicians
* heart areas affected by reduced circulation
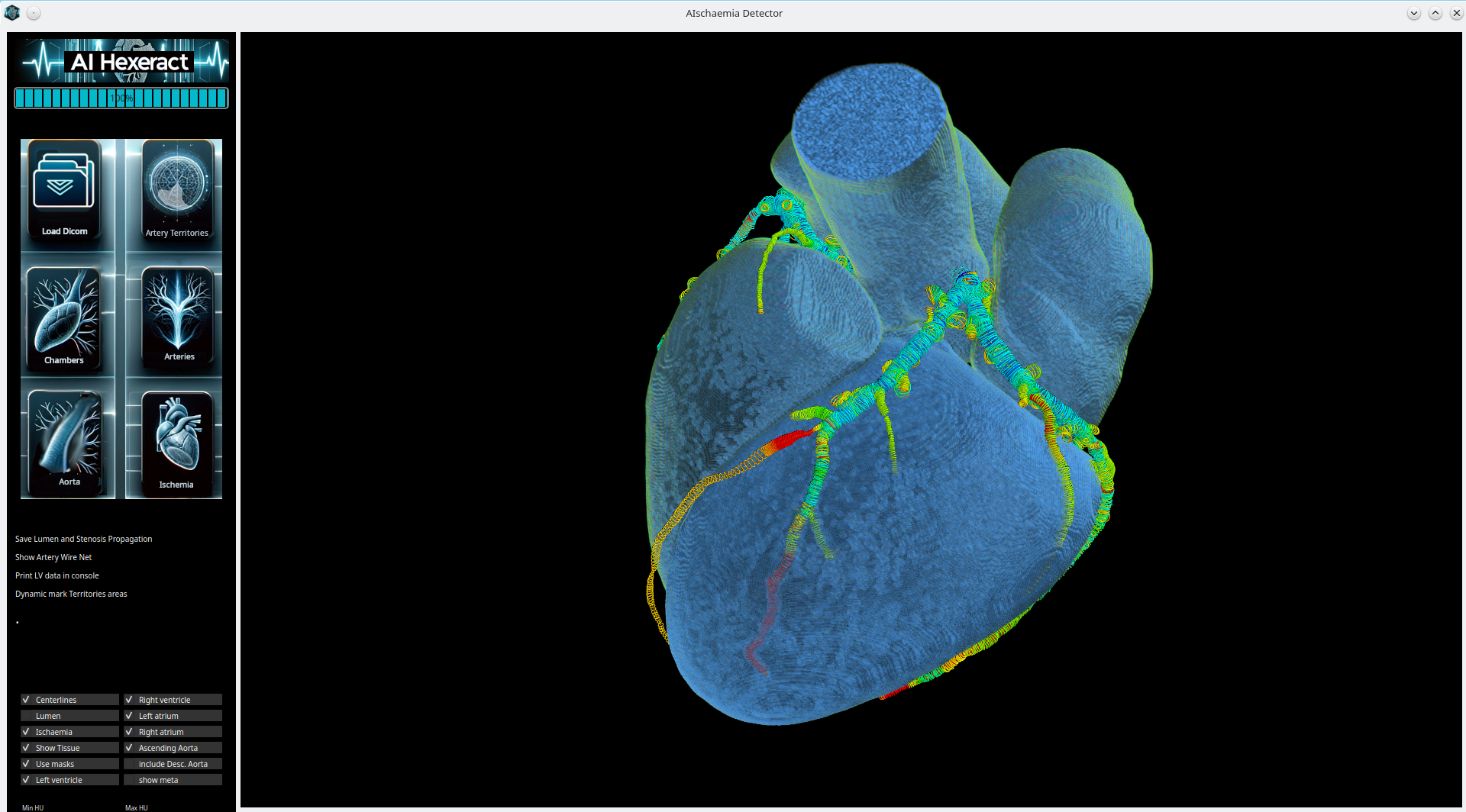
We infer voxel‑level ischaemic burden directly from standard CCTA. A GPU‑accelerated pipeline segments cardiac anatomy,
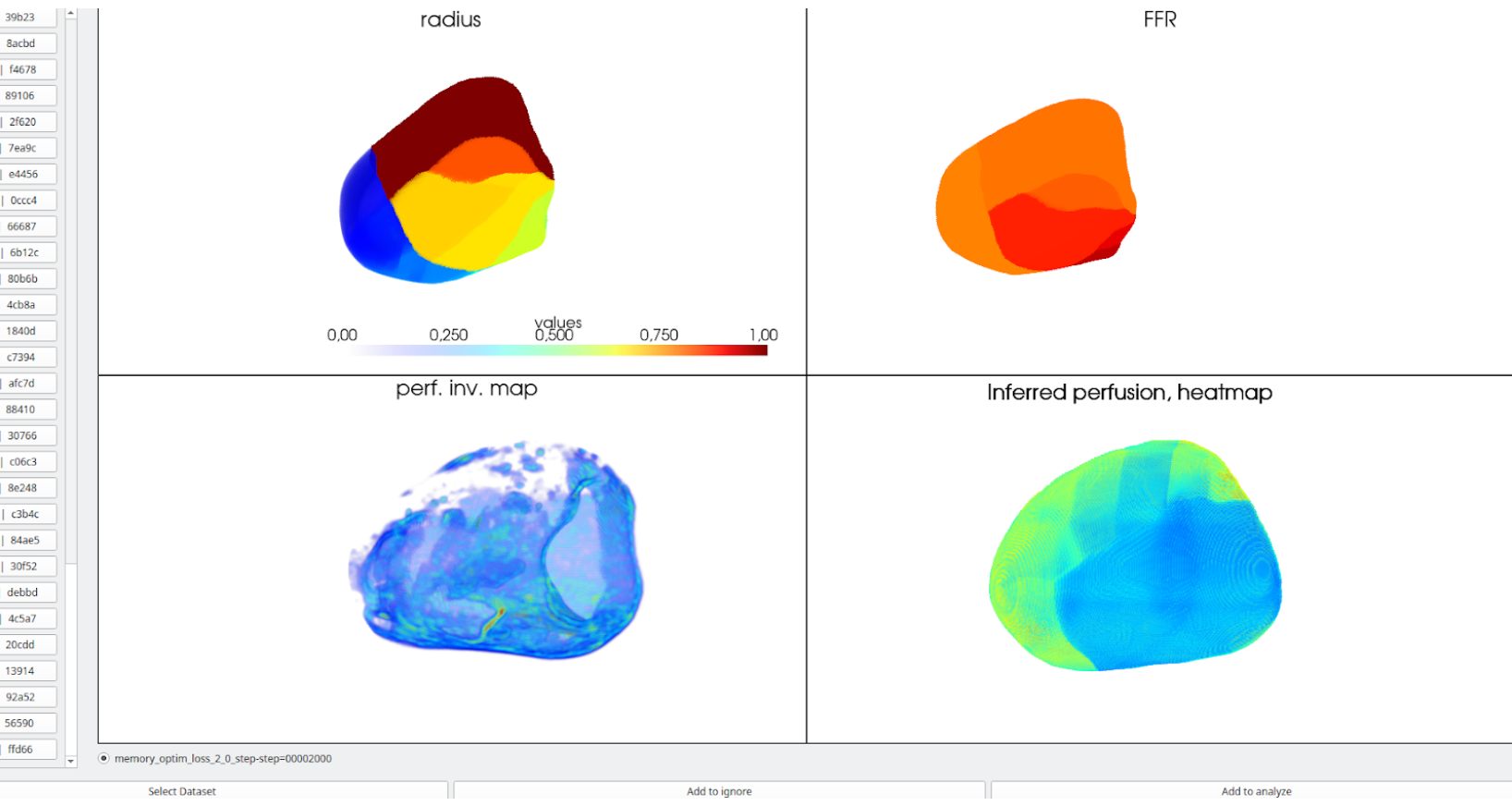
computes node‑level FFR along the coronary tree, projects vessel signals to branch‑weighted myocardial territories,
and localizes perfusion deficits with a novel 3‑D GAN trained on multimodal ground truth.
We’re preparing a $3M pre-Series A to fund clinical validation, MDR/FDA clearance, and first reimbursed deployments in cardiology centers.
r ≈ 0.85
Perfusion correlation (n=30)
65 s
Mean per‑case inference time
on H200 workstation
Pipeline Overview
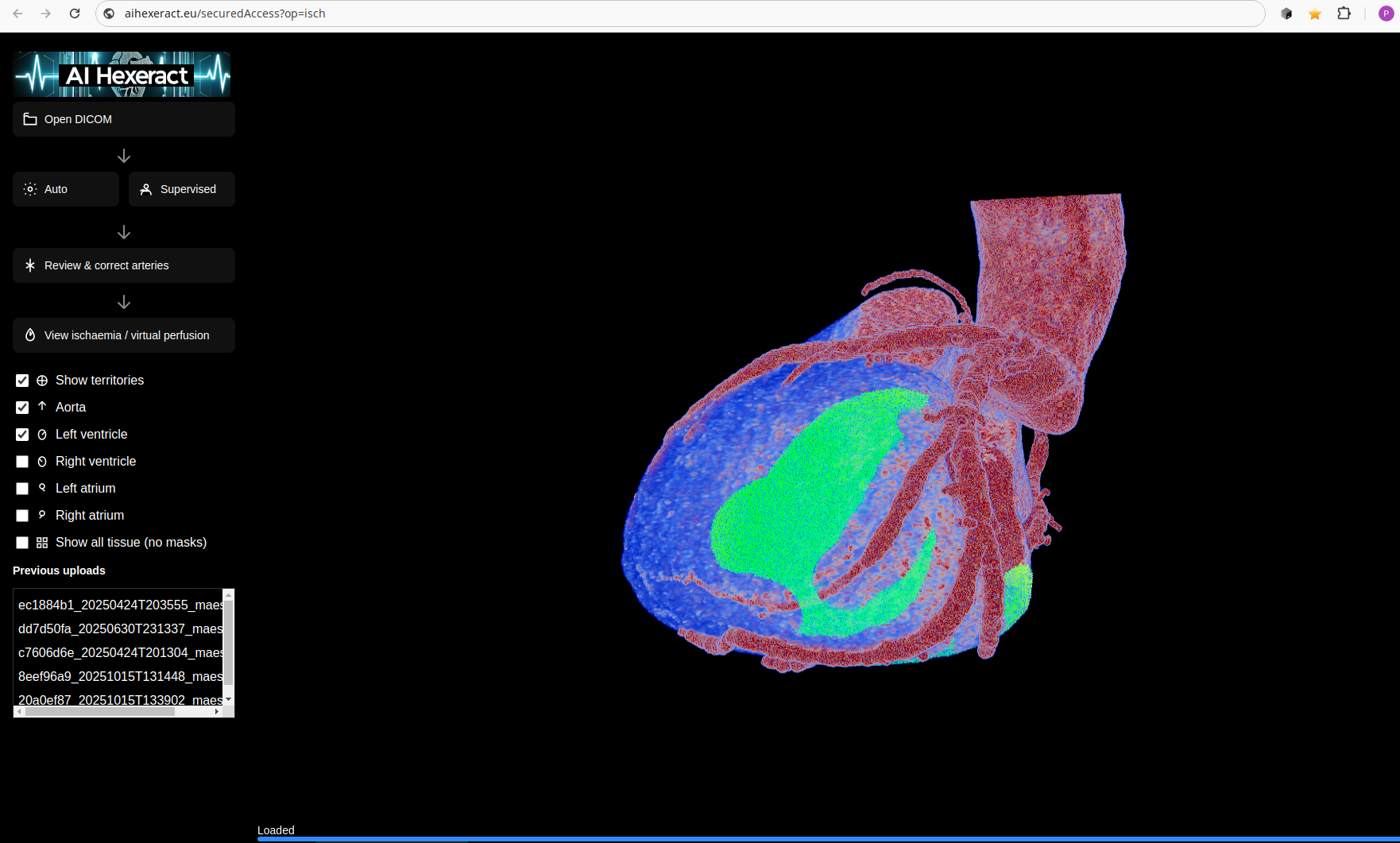
→ Inputs: standard Coronary CT Angiography (CCTA).
→ Segmentation: neural networks identify heart chambers, artery centerlines, and detailed lumen geometry.
→ FFR: stacked networks predict node‑level FFR along the coronary tree.
→ Territories: branch‑weighted Voronoi assignment projects vessel signals to myocardium.
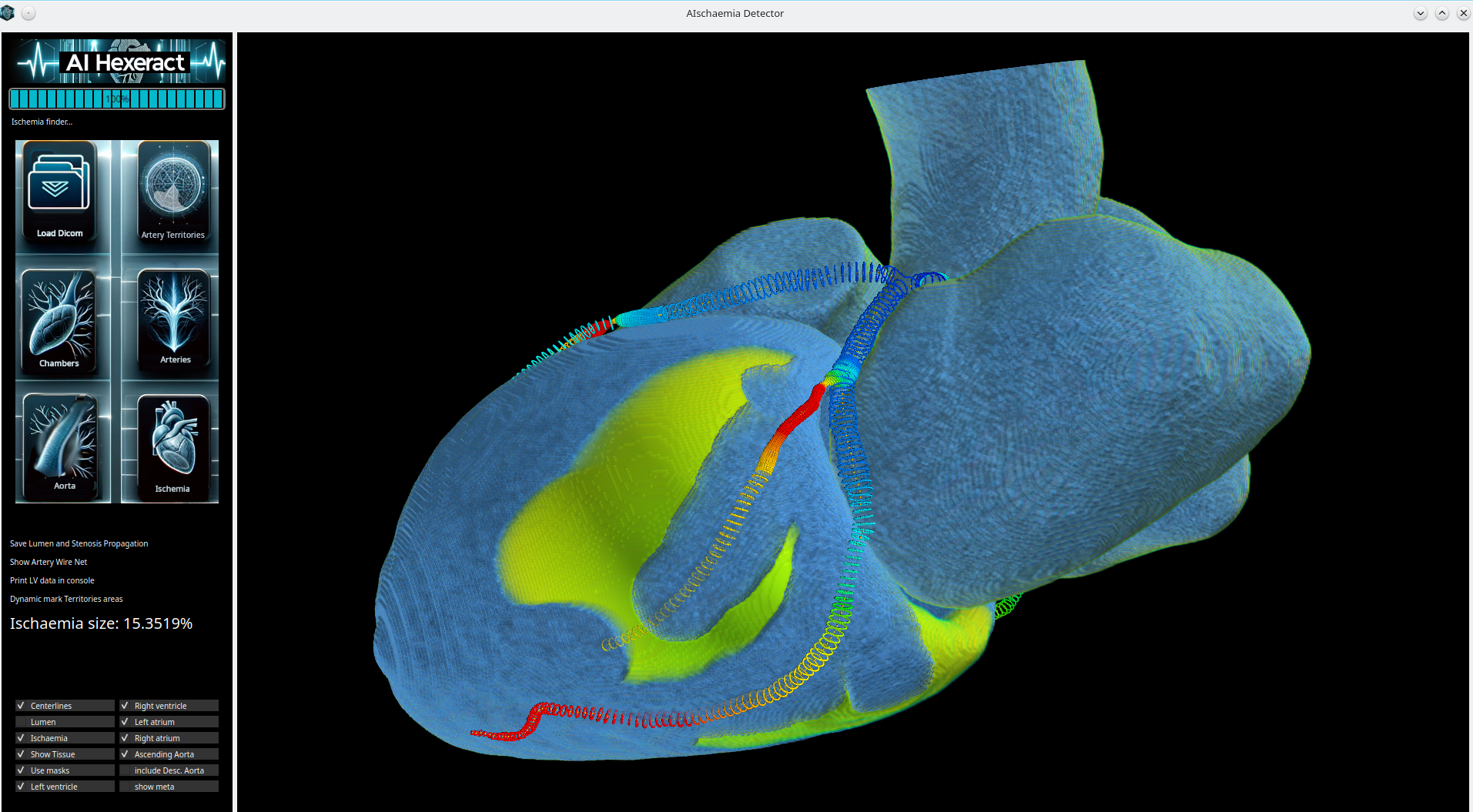
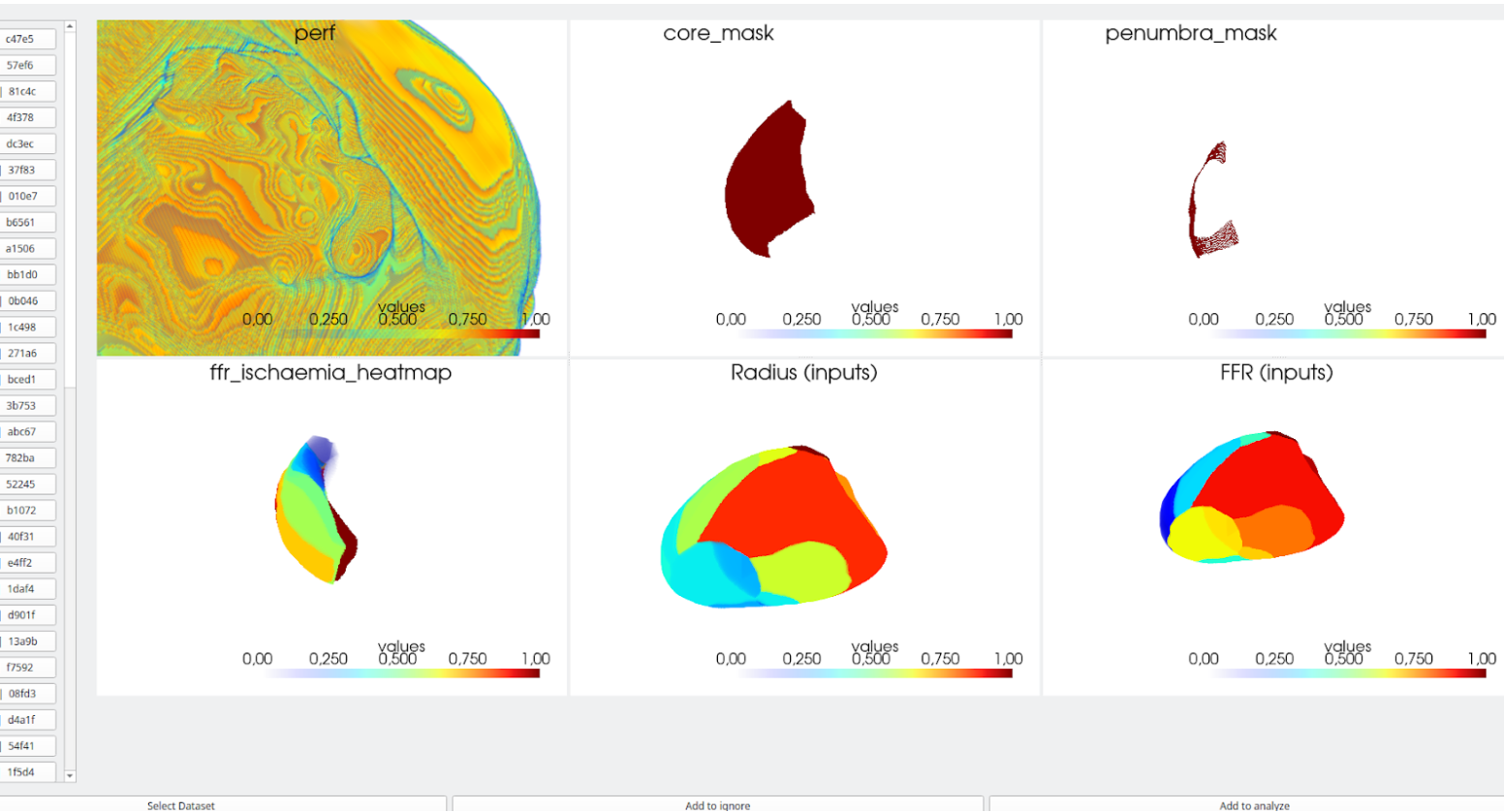
→ Ischaemia: a novel 3‑D network localizes & quantifies voxel‑level ischaemic burden.
What We Deliver
A fully GPU‑accelerated inference stack that transforms CCTA anatomy into actionable functional insights. Node‑level FFR supports lesion‑specific assessment, while voxel‑level
perfusion maps quantify the ischaemic core and penumbra across territories.
- Rapid analysis per case (~23 s segmentation, ~15 s artery analysis, ~2 s FFR, ~25 s ischaemia burden).
- Patient‑level validation with strict data hygiene.
- Explainable intermediates: vessels → territories → perfusion/ischaemia.
- Vendor‑agnostic integration with existing CCTA workflows.
Data & Cohorts
Total: 230 patients — 200 development, 30 validation. Stratified by FFR severity bins (<0.70, 0.70–0.80, >0.80). No cross‑patient leakage.
Preprocessing (including scaling) is fit on the development set and applied to validation only. Metrics are aggregated at the patient level to mirror clinical
deployment.
Methods at a Glance
- Split: Patient‑level; stratified by vessel/FFR bins; no study leakage.
- Metrics: FFR MSE/MAE/R²; voxel‑wise correlation within ROI; territory‑level AUC with sensitivity/specificity at pre‑declared
threshold.
- Calibration: reliability curve & ECE for FFR; Bland–Altman for perfusion.
- Stratification: per‑vessel (LAD/LCx/RCA), BMI bins, scanner/vendor subsets.
- Runtime: batched GPU inference; mixed precision; total 65s/case on H200‑class GPU.